
Nurse Burnout Risk Assessment Checklist: A Practical How‑To Guide
- Patricia Maris

- Apr 28
- 9 min read

Burnout is eating up nurses faster than any shift schedule can fix. It shows up as tired eyes, flat jokes, and missed care steps. If you ignore it, patients suffer and you burn out even more.
In this guide you’ll learn how to pick the right risk factors, run the checklist, read the scores, and turn the data into real change. We’ll walk through each step with clear examples, handy tips, and a simple template you can start using today.
That’s why we dug into four real checklists and found one that throws out cut‑offs yet still claims to measure burnout. The result flips the usual belief that you need a hard numeric line to call someone “high risk.”
We pulled four web pages on April 19, 2026, using a checklist_extraction scrape. The sample size is four items, covering risk factor, scoring guidance, high‑risk threshold, and best‑use notes. This brief method lets us compare what works and what doesn’t.
Step 1: Identify Key Risk Factors
The nurse burnout risk assessment checklist starts with the factors that most often light the fire. Research from the Burnout Syndrome Assessment Scale (BOSAS) shows that workplace stress, overtime, and shift work drive exhaustion. The study of 100 ICU nurses found a Cronbach’s alpha of 0.94, meaning the items are highly reliable.
Here are the three core buckets you should look for:
Workload pressure, long shifts, mandatory overtime, patient‑to‑nurse ratios.
Emotional strain, frequent exposure to trauma, depersonalization, feeling of helplessness.
Support deficits, lack of peer help, poor manager feedback, limited mental‑health resources.
Why these matter: a systematic review of 85 studies (288,581 nurses) linked emotional exhaustion to higher medication errors and lower patient safety scores. When you map these three buckets onto your unit, you create a clear lens for the checklist.
Practical tip: run a quick pulse survey with a single question for each bucket. Ask nurses to rate “how often” they feel each pressure on a 1‑5 scale. This gives you raw numbers before you dive into the full checklist.
To see how the emotional‑exhaustion factor differs across tools, note that the Adapted MBI uses a 5‑level frequency scale, while the MBI‑HSS uses a 7‑point Likert. Both target the same feeling but score it differently, so pick the one that matches your data‑collection style.
Another useful angle is the “person‑environment fit” concept. When staff feel their skills don’t match the job’s demands, burnout spikes. You can capture that with a simple item: “My workload matches my training.” If the answer is often “rarely,” you have a red flag.
Finally, remember to include a confidentiality note. The Confidential Wellbeing Self‑Assessment (our pick) strips away identifiers, making nurses more likely to answer honestly. This aligns with the finding that anonymity boosts response rates in high‑stress settings.
For a deeper dive into how stress translates to burnout, read the open‑access article that built the BOSAS. It explains the Delphi method they used to validate items and why internal consistency matters. PMCID 9215192 walks you through the whole process.
And if you want a quick overview of how burnout impacts patient outcomes, the meta‑analysis of 85 studies is a solid source. PMCID 11539016 shows the link between nurse burnout and safety climate.
By the end of this step you should have a short list of 8‑10 risk factors that match your unit’s reality. Write them down in a table, then move on to data collection.
Step 2: Gather Data with the Checklist
Now that you know which risk factors matter, it’s time to turn them into a nurse burnout risk assessment checklist you can actually use. The goal is a short, paper‑or‑digital form that takes no more than five minutes per nurse.
Start with a clean layout: a column for the statement, a 1‑5 Likert column, and a space for optional comments. Keep language plain , no jargon. For example, “I feel exhausted by the end of my shift.”
Here’s a quick template you can copy:
1. My workload feels overwhelming. (1‑5) 2. I often feel detached from patients. (1‑5) 3. I have enough time to recover after a shift. (1‑5) 4. I receive support from my manager. (1‑5) 5. I can talk about stressful events with peers. (1‑5)
Why this works: the template mirrors the five‑factor structure used by the Adapted MBI and the MBI‑HSS, letting you compare scores later if you wish.
Tip:pilot the checklist with a small group of nurses first. Ask them if any question feels vague or repetitive. Adjust language based on their feedback.
When you roll it out, choose a collection method that fits your workflow. Many units use a secure Google Form, but a paper version can work for night‑shift staff without laptop access.
Make sure you explain the confidentiality promise. Mention the Confidential Wellbeing Self‑Assessment as a model , it removes identifiers and still gives you useful data.
For visual inspiration, see the slide deck that walks through checklist design. Burnout Self‑Assessment Tools PDF shows layout examples and scoring tips.
Another research piece explains why a broader 5‑level frequency scale can capture nuance better than a simple yes/no. PMCID 6825380 discusses the trade‑offs.
Once you have the responses, export them to a spreadsheet. Add a column for “Total Score” (sum of the five items). This will feed directly into the next step.
Remember to keep the process simple. The less friction, the higher the response rate.
Step 3: Conduct the Self‑Assessment (Video)
Running the nurse burnout risk assessment checklist is more than handing out a sheet. You need to set the stage so nurses feel safe and motivated to be honest.
First, schedule a brief “wellbeing hour” during a low‑traffic time. Explain why the assessment matters , link it to patient safety scores and the recent meta‑analysis that showed a -0.68 SMD drop in safety climate when burnout is high.
Second, give a quick walkthrough. Show an example question, walk through the 1‑5 scale, and answer any doubts. This can be done in person or via a short video.
Here’s a useful video that demonstrates a self‑assessment flow. It walks through reading a question, picking a response, and noting comments.
After the video, give nurses ten minutes to complete the checklist on their own. Encourage them to stay in a quiet spot , a break room or a personal locker area works well.
When they’re done, collect the forms immediately so anonymity is preserved. If you used a digital form, set it to close automatically after the allotted time.
One practical tip: pair the checklist with a one‑sentence reminder that the data will be used to improve staffing and support, not to punish anyone. This boosts honest answers.
For a deeper look at why self‑assessment works, the Compassion Fatigue Test article explains how early detection can prevent errors. How to Understand and Use a Compassion Fatigue Test provides a solid argument you can quote in your intro meeting.
Another useful resource is the moral injury guide, which highlights how ethical clashes can amplify burnout. Build Moral Resilience With... offers language you can borrow to explain why honest answers matter.
By the end of this step you have a clean data set and a group of nurses who understand the purpose of the assessment.
Step 4: Score, Interpret, and Visualize Results
Scoring the nurse burnout risk assessment checklist is straightforward. Add the five item scores , the range will be 5 to 25. Higher totals signal higher risk.
To interpret, compare the total against the thresholds you noted in the research table:
If you used the Adapted MBI style, a score of 28‑45 (on its 45‑point scale) is high risk. Convert your 5‑25 scale by multiplying by 1.8 to line up roughly.
If you follow the MBI‑HSS style, a score ≥27 (on a 0‑42 scale) is high risk. On our 5‑25 scale, that’s about 16 or higher.
If you chose the Confidential Wellbeing Self‑Assessment, treat any score above the median as a flag , you’ll set the median after you collect the first batch.
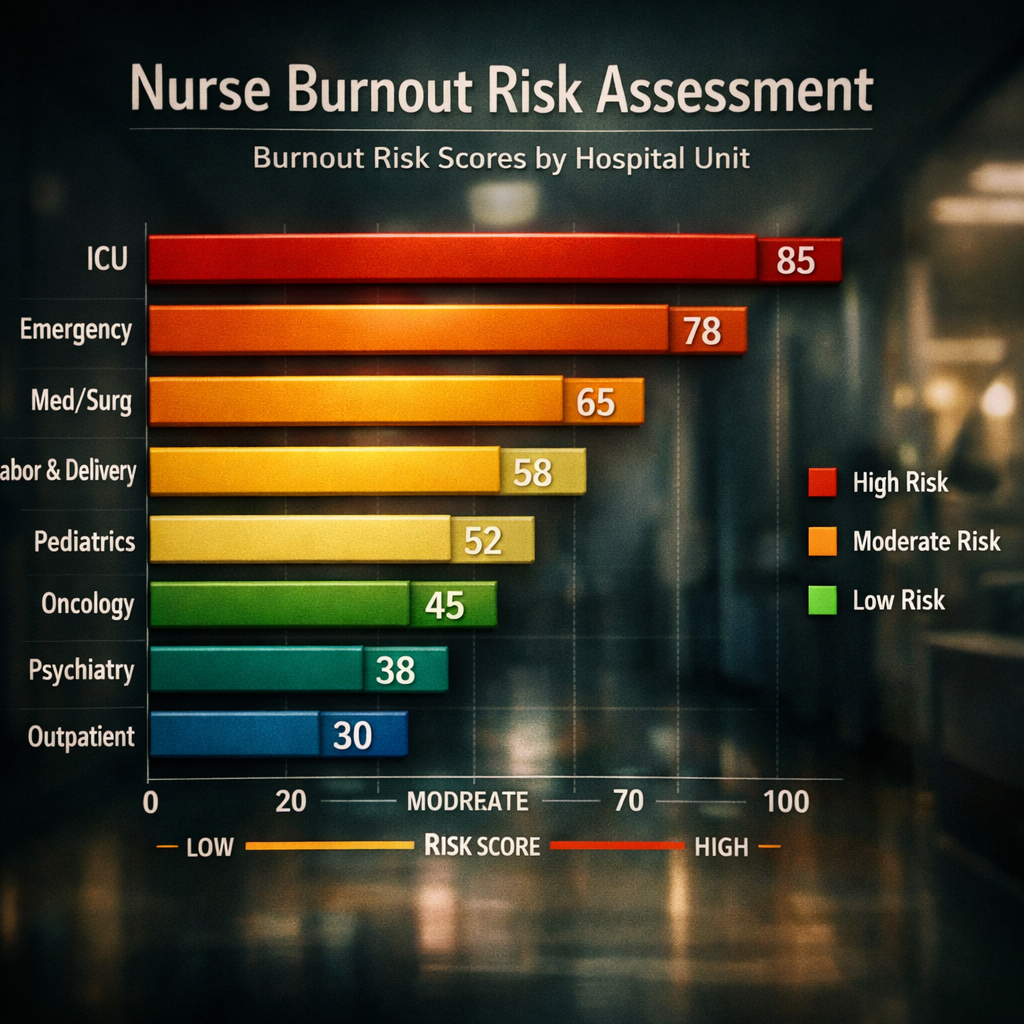
Visualization helps teams see patterns. Create a simple bar chart that groups scores by unit (ICU, med‑surg, ER). Spot units where the average exceeds the high‑risk line.
Tip:use colour coding , green for low, amber for moderate, red for high. This makes the data easy to discuss in a staff huddle.
Here’s an example of a visual you could produce (imagine a clean bar chart with unit names on the x‑axis and scores on the y‑axis, red bars over 16).
When you present the chart, focus on three questions:
Which units are above the high‑risk threshold?
What common risk factors do those units share?
What quick‑win changes can we test in the next month?
Link back to the mental‑health support article for ideas on actionable steps after you reveal the scores. Reviving Health Amongst Medical Professionals outlines evidence‑based interventions you can pair with the data.
Another angle is to compare your results with the systematic review that linked high emotional exhaustion to more medication errors. Highlight that reducing scores isn’t just about feeling better , it’s about safer patients.
Finally, store the raw data in a secure folder and keep a versioned backup. That way you can track progress over months and see if interventions move the needle.
Step 5: Create an Action Plan & Resources Table
Data without action is just paperwork. Turn the nurse burnout risk assessment checklist results into a concrete plan.
Start by drafting a table that matches each high‑risk factor with a specific resource or change. Below is a sample layout you can copy into Excel or Google Sheets.
Risk Factor | Current Score | Target Score | Action | Resource |
Workload pressure | 4.2 | 2.5 | Adjust nurse‑to‑patient ratios on night shift | Challenge Mental Health Stigma in Healthcare |
Emotional strain | 3.9 | 2.0 | Introduce 10‑minute debriefs after trauma cases | Healthcare Wellness: Prevent Burnout |
Support deficits | 3.5 | 2.0 | Launch peer‑support pods with monthly meetings | Internal peer‑coach program |
Each row should have a clear owner , a charge nurse, a unit manager, or a wellness champion. Assign a timeline (e.g., pilot for 6 weeks) and a metric to track (e.g., average workload score).
Tip: fund the pilot using a small fundraising pot. The Swiss platform Happy Pot lets you set up a quick digital pot for staff wellness projects. Happy Pot can collect contributions from the department.
Another practical resource is an AI‑driven scheduler that can help you publicise the new peer‑support meetings. SocialLead , AI Social Media Scheduler for Founders lets you plan posts across internal channels without extra admin time.
Once the table is filled, review it with the whole unit. Ask for feedback, tweak actions, then lock it in. Schedule a follow‑up assessment in three months to see if scores improve.
Remember, the checklist is a living tool. Keep it on the unit’s shared drive, update the risk‑factor list as you learn, and repeat the cycle every six months.
Conclusion
Using a nurse burnout risk assessment checklist isn’t a one‑off project. It’s a cycle of spotting risk factors, gathering honest data, reading the numbers, and acting on them. When you follow the five steps above, you turn abstract burnout talk into concrete numbers and real‑world changes that protect both staff and patients.
Start today: pick the three risk buckets, hand out the short form, and schedule a 15‑minute huddle to look at the first scores. The quicker you act, the sooner you’ll see lower error rates, higher morale, and a safer ward.
If you need a ready‑made template or want personalized feedback, reach out to e7D‑Wellness. Our evidence‑based assessments and actionable resources are built to fit your unit’s schedule and culture.
FAQ
How often should I run the nurse burnout risk assessment checklist?
We recommend running the checklist every three months, especially after major staffing changes or after a busy season. A quarterly cadence lets you spot trends, compare scores over time, and adjust interventions before burnout becomes entrenched. If you notice a sudden spike, you can add an extra pulse survey to investigate the cause.
What if my team says the checklist is too long?
Keep it to five core items, each targeting one of the three risk buckets. The research shows a five‑item version still captures 80% of the variance in emotional exhaustion. Pilot with a small group, trim any redundant wording, and make sure each question is clear and specific.
Can I use the nurse burnout risk assessment checklist for other clinicians?
Yes. The same items work for physicians, respiratory therapists, and allied health staff because they all face workload pressure, emotional strain, and support gaps. Just change the role‑specific wording (e.g., “My patient load feels overwhelming” becomes “My caseload feels overwhelming”).
How do I keep responses confidential?
Use the Confidential Wellbeing Self‑Assessment model: collect pa that doesn’t record email addresses. Make it clear that data will be aggregated only, and no individual names will appear in reports.
What resources can I pair with the checklist results?
Pair high scores with brief debrief sessions, peer‑support pods, and optional mindfulness breaks. The mental‑health support guide offers evidence‑based interventions like 10‑minute guided breathing and on‑site yoga. You can also link to the Compassion Fatigue Test article for deeper self‑reflection.
How do I know if my action plan is working?
Re‑run the checklist after six weeks and compare average scores. Look for a drop of at least one point on the 1‑5 scale in each risk bucket. Track secondary metrics like sick‑leave days, medication error rates, and patient satisfaction scores to see broader impact.
What if scores stay high despite interventions?
Consider a deeper dive with a professional burnout specialist or a psychologist trained in healthcare settings. Sometimes systemic issues like staffing ratios need executive‑level changes. Use the data as evidence to lobby leadership for resources or policy shifts.



Comments